Case report publication – Germany, 2. 2018
Journal – TeamWork Dentales Journal 2. 2018
Introduction
An anticipated implant-supported prosthetic restoration of the edentulous patient often presents the treatment team with considerable challenges. Both the restoration of aesthetics and function should be taken into account. Surgical components of a comprehensive treatment plan include number, position and orientation of the necessary implants. On the other hand, there are many options for the definitive prosthetic restoration; a wide range of different heterogeneous materials are available today. Digital planning of the prosthetic restoration and the use of high-quality CAD-CAM milled restorations made of prefabricated polymers in disc form offers considerable advantages and is increasingly the focus of modern implant prosthetics. In the clinical case presented, advantages of digital planning in the laboratory and milling of primary and secondary parts in LuxaCam PEEK come to the fore as a high-quality and elegant definitive prosthetic solution.
Case presentation
The 82-year-old retired orthopaedic surgeon is presented in our practice with the desire for an implant-supported removable restoration in the upper jaw. His few remaining teeth were removed 6 months ago; he now wears a denture. He is not satisfied with the hold of the existing prosthesis; thus, the fabrication of a new implant-supported removable prosthesis in the maxilla is indicated. His wish is to be treated surgically and prosthetically in a minimally invasive manner using state-of-the-art digital dental technology.
Clinical treatment steps
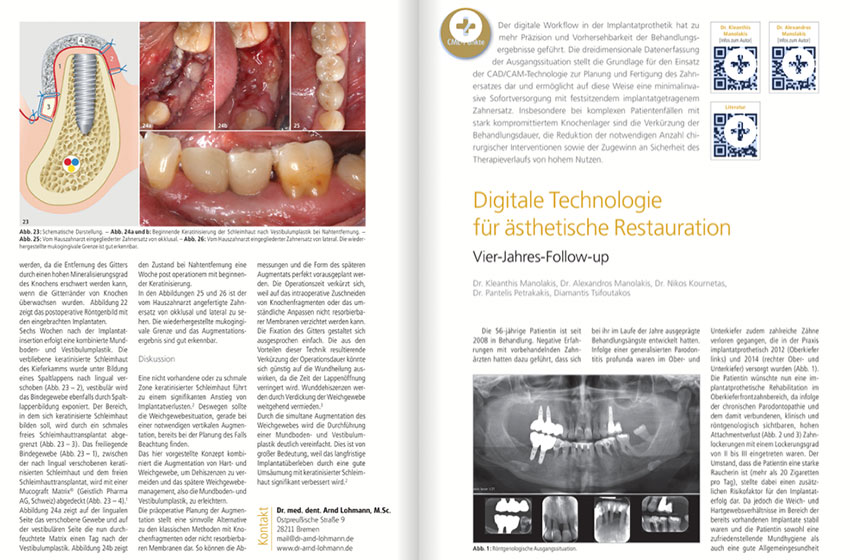
The existing denture in the upper jaw satisfactorily meets functional and aesthetic aspects. Thus, this prosthesis serves as an optimal starting point for the definitive restoration. The existing prosthesis is copied in the laboratory and an identical scan prosthesis is used to create a DVT imaging. A digital volume tomography is the first indispensable digital step to determine existing bone supply in the upper jaw and at the same time to decide on number, size, dimension and orientation of necessary dental implants.
Based on prosthetic and surgical criteria (existing bone availability in the upper anterior and posterior area, jaw relation, minimally invasive surgical concept with a reduced number of implants and transgingival implant insertion) the treatment team decided on four implants placed symmetrically on both sides in the first premolar and first molar region. In this way a sufficient hold of the definitive hybrid prosthesis is achieved. At the same time the upper anterior region is spared from implants, for maximum volume reduction of the reconstruction in this phonetically sensitive region. A surgical template for the navigated implant placement was then digitally designed and printed in the dental office. This printed template was provided with retention pins so that the mucosa-supported template can be held particularly securely during surgery. Four BEGO Semados titanium implants are thus quickly, precisely and minimally invasively inserted transgingivally into the jawbone.
After an uncomplicated 2-month period of covered osseointegration, implants were uncovered from the covering mucosa with minimal incisions and open tray impression was taken conventionally in the same session using Honigum Heavy (DMG Hamburg). Honigum Heavy is characterized by ideal flowability, high detail reproduction and at the same time optimal final hardness.
Dental laboratory sequence
After the conventional hard plaster model has been provided with the corresponding scan posts, digital scanning takes place in the laboratory scanner. Initially the two bars are designed digitally on the screen, then one can continue with digital planning of the mesiostructure. Digital planning in the laboratory offers extensive freedom. With digital planning, one has a lot of leeway to decide in advance about correct and sensible dimensions of the matching parts. In addition, of course one has the option of designing the mesiostructure thinner or thicker as required using the superimposed scanned dimensions of the definitive restoration. After the lab technician is satisfied with the design of the prosthetic units, bars and mesiostructure can be milled from a PEEK disc in the laboratory. When milling is completed PEEK bars are finished and bonded to the Ti-bases using adhesive composite cement. They are then provided with extracoronal ball attachments on the mesial and distal end. The extracoronal ball anchors matrices are glued to the PEEK framework and serve as additional retention if clinically necessary. PEEK framework is veneered with high-quality denture teeth and denture resin and delivered to the dentist for intraoral try-in.
Clinical steps
Bars are now screwed onto the implants intraorally and the removable prosthesis is tried in. When laboratory work is performed properly and precisely, hardly any corrections are usually necessary. The patient judged aesthetics and function of the supplied restoration to be very advantageous, prosthesis hold is convincing. The design and material used for this specific removable upper jaw prosthesis is particularly light, weighing less than ten grams. PEEK is also considered to be particularly beneficial in terms of plaque accumulation.
Conclusions
Digital planning of an extensive implant-supported restoration in the edentulous maxilla in the dental laboratory offers a number of advantages. One can flexibly and quickly carry out several levels of the planning process precisely and clearly. Creation of primary and secondary parts in one process from a PEEK disc in the sense of the CAD-CAM process accelerates the manufacturing process. Three-dimensional data of the restoration remain stored in the computer and the same prosthetic work can be repeated as required with dimensional stability. PEEK is considered to be a particularly light, tissue-friendly and stable novel restorative material. The presented process of creating an implant-supported hybrid prosthesis made of PEEK represents a cost-effective and modern restorative alternative.