Authors
K. Manolakis DDS, P. Petrakakis DDS, A. Manolakis DDS, D. Tsirakidis MDT
Date of Publication
Germany, February 2017
Organization
Dentale Implantologie & Parodontologie International, Spitta Publishing Group, Germany
Partial or total teeth loss is associated with reduced quality of life and psychosocial problems in most cases. In patients treated with conventional removable dental prostheses to replace missing teeth, gain in quality of life does not seem to be possible to the desired extent. The replacement of missing teeth with implant-supported restorations is therefore a preferred treatment option, since the attachment of prosthetic restorations on implants leads to a higher treatment satisfaction than conventional mucosa supported restorative options.
The central question is raised as to which type of connection between implant and superstructure and which type of restoration (fixed vs. removable, or conditionally removable) is suitable depending on the patient situation to achieve predictable treatment outcomes and long-term treatment success. Treatment success is defined not only from the point of view of the dentist; patient satisfaction, the manageability or care ability of the new dental prosthesis as well as economic aspects must also be taken into account. Treatment success obviously depends to a greater extent on how the patient perceives the treatment result from his point of view and not exclusively how the success of the therapy is defined and perceived by the practitioner. A minimally invasive approach without extensive augmentation is in this context a treatment option favored by the majority of patients. It is of interest to what extent an implant restoration is actually possible in patients presenting bony alveolar process resorption without bone augmentation and how many implants are necessary to achieve a satisfactory rehabilitation.
Implant treatment therefore focuses on both objective functional parameters, such as the long-term rehabilitation of chewing and / or speaking ability, as well as patient-specific, psychosocial factors, such as improved quality of life and improved aesthetics. It can not always be ruled out that the patient’s expectations regarding his prosthetic rehabilitation can not be met; therefore, it is appropriate to use implant systems that allow multiple treatment options simultaneously and are thus independent of the ultimate decision on the design of the suprastructure and the type of fixation and that allow modifications of the original design of the prosthetic restoration during ongoing therapy. In the case of a reduced budget, patients can initially be provided with a removable treatment option and thus be provided with cheaper care. If the patient’s economic situation permits, the removable solution can be easily converted into a higher-quality, fixed prosthetic option. Conversely, this approach also has the advantage of being able to resuscitate patients with a removable implant-supported prosthesis as they age, which leads to a potential for increased loss of hygiene.
Comparison of various attachments for implant supported restorations on four implants in the edentulous jaw – a case report.
Authors
Partial or total loss of teeth is associated with reduced quality of life and psychosocial problems in most cases [1, 2]. In patients treated with conventional removable dental prostheses to replace missing teeth, gain in quality of life does not seem to be possible to the desired extent [3]. The replacement of missing teeth with implant-supported restorations is therefore a preferred treatment option, since the attachment of prosthetic restorations on implants leads to a higher treatment satisfaction than conventional mucosa supported restorative options [4-9].
This raises the central question as to which type of connection between implant and superstructure and which type of restoration (fixed vs. removable, or conditionally removable) is suitable depending on the patient situation, to achieve predictable treatment outcomes and long-term treatment success. Treatment success is defined not only from the point of view of the dentist. The satisfaction of the patient, the manageability or care ability of the new dental prosthesis as well as economic aspects must also be taken into account in the intended treatment outcome [10]. The success of a treatment obviously depends to a greater extent on how the patient perceives the treatment result from his point of view and not exclusively how the success of the therapy is defined and perceived by the practitioner [11].
A minimally invasive approach without extensive augmentation is in this context a treatment option favored by the majority of patients [4, 12]. It is of interest to what extent an implant restoration is actually possible in patients presenting bony alveolar process resorption without bone augmentation and how many implants are necessary to achieve a satisfactory rehabilitation.
Implant treatment therefore focuses on both objective functional parameters, such as the long-term rehabilitation of chewing and / or speaking ability, as well as patient-specific, psychosocial factors, such as improved quality of life and improved aesthetics [13]. In order to take the patient’s preferences into consideration and at the same time not jeopardize the treatment success, a thorough communication between the dentist and the patient is essential [14, 15].
Despite good communication between the patient and the practitioner, it can not always be ruled out that the patient’s expectations regarding his prosthetic rehabilitation can not be met [16-18]. Therefore, it is appropriate to use implant systems that allow multiple treatment options simultaneously and are thus independent of the ultimate decision on the design of the suprastructure and the type of fixation and that allow modifications of the original design of the prosthetic restoration during ongoing therapy [18]. In the case of a reduced budget, patients can initially be provided with a removable treatment option and thus be provided with cheaper care. If the patient’s economic situation permits, the removable solution can be easily converted into a higher-quality, fixed prosthetic option. Conversely, this approach also has the advantage of being able to resuscitate patients with a removable implant-supported prosthesis as they age, which leads to a potential for increased loss of hygiene.
This fact has already been recognized by components manufacturers. For example, the company BEGO Implant Systems (Bremen, Germany) offers implant systems that can be equipped flexibly with different prosthetic abutment and connection systems.
Flexibility is especially important in light of the fact that no generally valid recommendations can be made from the currently available statements in the literature as to which therapy option for treatment with implant-supported restorations is the treatment of choice. The number of implants or the type of connection between implants and the superstructure do not seem to have an impact on oral quality of life, as a retrospective comparative clinical study has shown [19]. However, the results of another clinical study showed that this result is not universal with respect to the type of prosthetic connection. There, interforaminal implants placed in the lower jaw by means of bars led to a significantly better perceived oral quality of life than implants without bar connections [20]. Additionally, number of implants and the type of prosthetic attachment had no influence on patient satisfaction.
The findings show that objective parameters, such as the success or survival rates of implants and prosthetic superstructures also do not seem to depend on the number of implants. In most clinical cases, the fixation of implant-supported supraconstructions in the lower jaw, varying from minimally two [21] or a maximum of four to six implants, may be considered as a suitable and predictable treatment option [22-25].
In implant prosthetic and laboratory terms, having fewer implants has the advantage of facilitating parallel insertion on the patient and parallelization in the laboratory as well as fabrication of the superstructure is simplified.
The principle of using a reduced number of implants was implemented in the All-on-4® concept, which was already developed by Paolo Maló in the late 1990s. This procedure allows a minimally invasive approach to immediate restoration with fixed provisional or definitive dentures on a reduced number of implants. In the lower jaw, the interforaminal region can be considered as a preferable insertion site for this type of restoration, as there is usually the largest supply of bone and there is no risk of injury to the inferior alveolar nerve when placing implants.
The two proximal implants are inserted straight while the distal implants are inserted at an angle, in order to obtain the largest possible support polygon for the prosthetic superstructure. The inclination of the distal implants is then corrected with specially designed angulated abutments. The apparently small influence of the number of implants and the nature of the connection to the superstructure on functional and psychosocial parameters are also reported in two randomized clinical investigations by Krennmair et al. There, an improvement in patient satisfaction was also achieved in the stabilization of mandibular prostheses on only two implants. After one or five years on function no implant loss was observed [26, 27]. In the same studies, the type of connection between implant and prosthetic superstructure (ball attachment vs. locator) also had no influence on subjective patient preference or on objective implant-related clinical and radiographic parameters [26].
Objective of the case report
The objective of the present case report was to test out different prosthetic restoration concepts for implant placement without augmentative measures on a single patient. On the basis of this procedure, it was to be determined to what extent attachment systems are actually interchangeable without much effort. Locator®-like abutments (PS Easy-Con, BEGO Implant Systems, Bremen, Germany) and ball attachments (PS BA, BEGO Implant Systems) were used for a removable prosthetic restoration. As a screw retained restorative option, a composite-veneered bridge was fabricated and fixed on MultiPlus abutments (BEGO Implant Systems), on a cobalt-chrome framework produced by means of selective laser melting SLM.
Initial situation
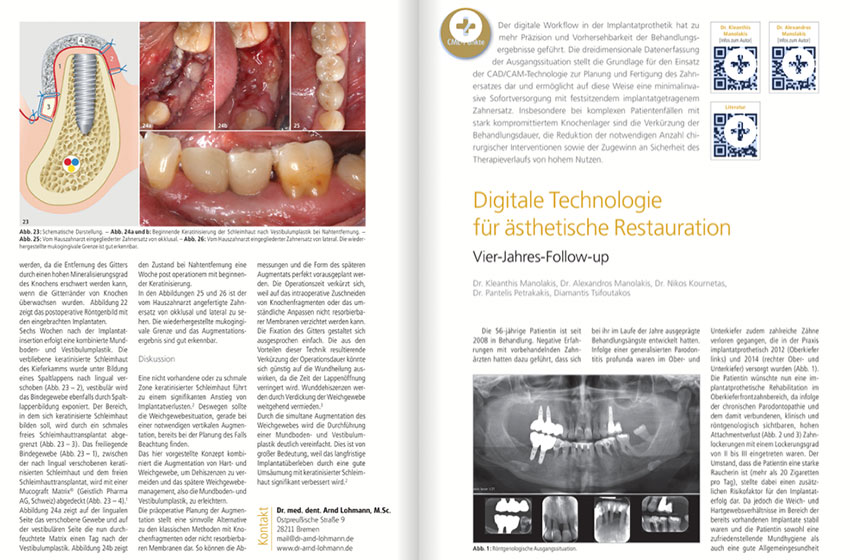
The 69-year-old male patient presented in our practice with the desire to be provided with an implant-supported restoration in the lower jaw. He had no systemic diseases, was a non-smoker and did not take any medications. The oral hygiene of the patient was average. He had the desire for an implant supported restoration, which should be minimally invasive and should be fixed on a reduced number of implants, without any augmentative measures. During the period of the last eight years he was restored with a removable partial denture, fixed by means of metallic clasp retaining elements on the only remaining tooth 33. Due to massive periodontal problems, the tooth was no longer worth preserving (Figs. 1 and 2). In the opposite jaw, the patient was provided with inadequate fixed crowns & bridges, which also should be renewed at a later date.
Fig. 1 and 2: initial OPG, periapical radiograph 33.
Basically, it is assumed that in the case of a residual alveolar bone smaller than 5.0 mm in width in connection with implant treatment, bone augmentation measures have to be performed in order to obtain a sufficiently sized bone bed for the implants [28]. In the present case, the alveolar process in the region of the insertion sites of the implants barely met the requirements of implantation without additional augmentation measures. We decided in consultation with the patient for the extraction of the tooth 33 and for a subsequent implant-supported prosthetic restoration of the lower jaw on four implants in the canine and molar area on both sides without additional augmentation measures.
The quality of mandibular alveolar bone was considered D3 according to Misch classification [29-31]. Bone of level D3 belongs next to the second highest quality level D2 to the
most commonly observed bone densities. In the literature it is described that in D1 and D4 bone the risk for early implant losses compared to the other two bone quality classes is increased [32]. Nevertheless, in view of the relatively limited amount of available bone, a two-step procedure with a delayed loading protocol and covered healing was chosen, to ensure sufficient implant stability in the alveolar bone over a healing period of several weeks. About three months after extraction of the tooth 33 surgical implant placement took place. Within this period, enough bone was formed in the area of the bony defect in tooth 33, so that implantation could also take place in this area (Fig. 3).
Initial situation, before elevating a mucoperiosteal flap for implant placement; healed #33 site
Surgical phase
Implant placement was performed under local anesthesia and under direct vision, with the formation of a mucoperiosteal flap. The open procedure was chosen as there was an advanced resorption of the bony alveolar process in the oro-vestibular direction, thus allowing a very good assessment of the bone contours and the quality of the bone as well as an implant positioning under direct vision [33-35]. BEGO Semados® RSX Implants (BEGO Implant Systems) with the standard diameters 3.75 mm (area #36 and #43) and 4.10 mm (area #46 and #33) were used. Implantation took place freehand according to the standard protocol of the manufacturer. All implants were placed epicrestally on the buccal aspect, with the exception of the implant in area #43 (Fig. 4). Since the alveolar crest was saddle-shaped, the implant neck was approximately 1.0 mm subcrestal for all implants approximately.
Due to the good vertical bone supply, implants with a length of 11.5 mm could be used in the canine area and implants with a length of 10 mm in the posterior area. In this case, it was not necessary to angulate the posterior implants – as is usual with the classic All-on-4® method (Fig. 5). Mucosa was sutured over the implants and the patient was instructed not to wear the prosthesis for a week. The one-week prosthesis course was prescribed to reduce the risk of mucosal perforation in the implant area and subsequent infection [36]. One week after implantation, the patient presented again for suture removal. Mucosa in the surgical area showed no signs of infection (Fig. 6).
Fig. 6: Complication-free healing 2 months after implant insertion
Fig. 7: Healing posts in situ two months after implant insertion
Prosthetic phase
After another 7-week healing period, the implants were uncovered and platform-shifting gingival formers were placed (Figure 7). Two weeks later, impressions were taken. After another two weeks, the patient’s definitive prosthetic restoration was performed.
Prosthetic connection elements for removable reconstructions
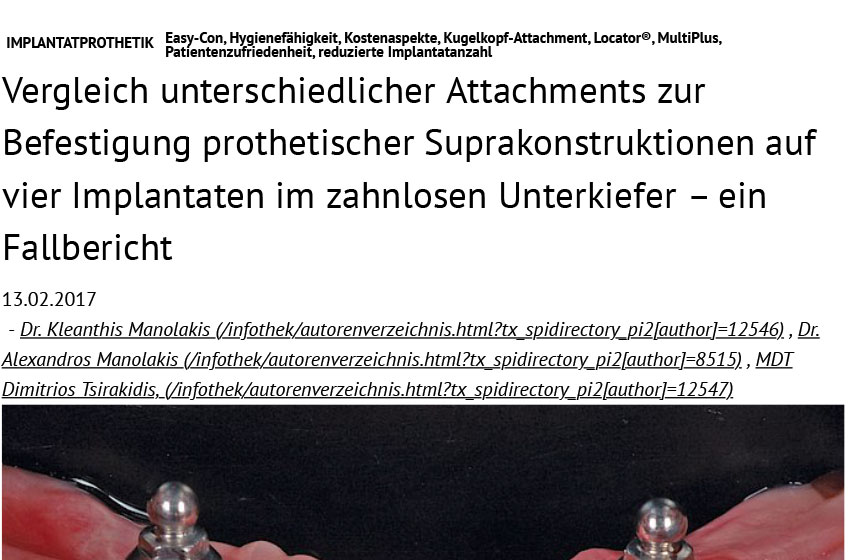
For the attachment of implant supported removable prosthetic reconstructions in this case report ball attachments and Locator®-like Easy-Con abutments (PS Easy-Con) were used. Ball attachments consist of a spherical metallic male part (Fig. 8). The matrix is incorporated into the prosthesis and may be made of metal or plastic (Figure 9). The advantages of ball attachments for retaining removable restorations are the good hygienic ability, the low costs and the reduced treatment time [7].
Fig. 8: Intraoral condition after fixing the four ball attachments.
Fig. 9: Matrices for the ball anchors incorporated in the prosthesis base.
A relatively high repair liability due to retention losses is compensated by the fact that repairs in this system can be carried out very quickly and easily. However, due to their height, ball attachments require a sufficient intermaxillary distance, which can complicate the design of the prosthetic restoration, since the anchor has a correspondingly large vertical space requirement and the attachment extends far into the oral cavity. Another disadvantage is that ball attachments can be used only on axially and parallel placed implants. Retention is significantly reduced on implants deviating from angulation> 15 degrees [7].
In this clinical case implants were positioned approximately parallel, so that there were no major deviations of the implant axes (Fig. 10). There was ample intermaxillary space and we were able to provide the patient with a removable denture fixed to ball attachments. Clinical outcomes were very satisfactory for the clinician and the patient, both visually and functionally (Figures 11 and 12).
Fig. 10: Relatively parallel positioning of the implants with small angular deviations.
Fig. 11: Cover denture prosthesis mounted on ball attachments in situ
Fig. 12: Good aesthetic and functional result of the cover denture prosthesis
The Easy-Con system is also susceptible to repair, as the replacement of the polyamide inserts must take place due to retention losses [26]. Since the restoration height is significantly lower than with the ball attachments, the Easy-Con abutments can be used very well as attachments where reduced intermaxillary distance is available. Easy-Con abutments consist of a metal matrix integrated in the abutment. This consists of a raised, annular edge. The polyamide (nylon) male is placed on the annular abutment and retains its retention over both the outer surfaces and the inner surfaces of the metal ring (Figure 13). The denture base contains polyamide inserts (Fig. 14). Due to the material-related elasticity of the Easy-Con components, this system has a favorable elasticity / resilience (self-aligning) and is able to adapt well to the movements of the superstructure during functional loading [7]. Compared to the ball attachment system, this design allows axial disparallelities between implants to be compensated up to a deviation angle of 40 degrees without loss of retention [37]. The patient was also successfully restored with a functional and visually appealing Cover denture prosthesis using the Easy-Con system (Fig. 15).
Fig. 13: PS Easy-Con abutments in situ.
Fig. 14: Easy-Con retention caps containing polyamide inserts are incorporated into the denture base.
Fig. 15: Final removable prosthesis on PS Easy-Con abutments in situ.
No significant differences in clinical or radiographic parameters could be identified between Locator®-like abutments and ball attachments in a clinical study after a five-year period under functional loading [27]. In the case of ball attachments, more frequent prosthetic aftercare was initially required compared to Locator®-like abutments, but these decreased with increasing observation time and no longer differed in the frequency of self-aligning systems.
In a more recent in-vitro study, statistically significant differences in the retention behavior and stability of a cobalt-chrome prosthesis framework fixed on two implants were determined depending on the respective prosthetic attachment system, the force applied and the distribution of implants / implant positioning. The highest retention and stability values were measured with ball-headed attachments, followed by self-aligning systems [38]. The further distal implants were placed, the higher retention and stability values were achieved in the anterior-posterior direction. When connecting Locator®-like abutments to four implants in the lower jaw using bars, lower crestal bone loss rates and reduced follow-up were found compared to simple Locator® system junctions on two implants [39]. The different effects on crestal bone resorption in this study were attributed to the stabilization effect through the bars rather than the type of prosthetic connection. In contrast, an older in vitro study showed that ball-headed abutments on implants lead to a better distribution of force in the lower jaw posterior region than bar connections [40]. In a clinical comparative study of the treatment of edentulous patients in the mandible using two implants and locators, magnetic attachments showed significantly lower peri-implant bone loss than locator attachments [41]. Based on the available evidence, it is not yet possible to make definitive statements on the influence of different prosthetic connections in implant-supported, removable dentures on the remodeling behavior of crestal bone.
Fixed implant-supported reconstructions
The third treatment option was a screw retained reconstruction attached to the native PS MultiPlus abutment (Figs 16 and 17). The basis for the conditionally removable bridge was a cobalt-chromium framework (EOS, Electro Optical Systems Munich, Germany) produced by means of selective laser melting. In our patient case, a very good, accurate fit of the metal framework could be achieved (Fig. 18). The framework was veneered using composite (anaxblend big block dentin and big block enamel, anaxdent GmbH, Stuttgart, Germany) (Figures 19a and b). The screw channels were sealed with composites (EcuSphere-Carat, DMG Chemisch-Pharmazeutische Fabrik GmbH, Hamburg, Germany) after the onset of the superstructure (Fig. 20). The final clinical outcome was very satisfactory for the patient as the reconstruction was very natural and aesthetic (Figure 21).
Fig. 16: PS MultiPlus abutments in situ.
Fig. 17: Close-up of the PS MultiPlus Abutment.
Fig. 18: Good fit of the SLM cobalt-chrome framework.
Fig. 19a: Finalized composite veneered bridge.
Fig. 19b: Composite veneered bridge in situ.
Fig. 20: Screw channels sealed with composite.
Fig. 21: Labial view of the implant-supported lower jaw bridge.
It is important that the patient is intensively instructed in the oral hygiene and cleaning of the implant supported restoration so as not to jeopardize the long-term success. This is of great importance, because patients are often unaware that implants require more care than natural teeth [42]. If it turns out that sufficient oral care is not possible, other attachments can be used in consultation with the patient and existing implant supported restorations can be made removable again.
Removable implant supported cover denture restorations are apparently less well accepted by patients than fixed implant-supported restorations [11, 43, 44]. The increased acceptance of fixed implant-supported superstructures can be attributed to the modified design of the prosthetic replacement, as the fixed restoration is designed as a bridge, veneered with ceramic or composite material, and lacks the plastic extensions required in the cover denture solution. Improved aesthetics and wearing comfort of fixed bridges compared to cover denture prostheses obviously also lead to increased patient satisfaction [11, 43, 44]. However, oral hygiene procedures in fixed reconstructions are more difficult to perform by the patient than is the case with removable prostheses. However, removable reconstructions appear to be more susceptible to repair than fixed dentures [45]. Regarding implant survival rates, in both fixed and removable supraconstructions, in contrast to the results of the examinations listed in the previous sections, there seems to be a significant dependency on the number of implants. A recent systematic review, including a meta-analysis, found that fixation of fixed reconstructions on four implants and removable dentures on two mandibular implants leads to higher implant loss rates than if more implants are used to stabilize the superstructures [46].
Retaining possibilities of the superstructure
Fixed implant supported restorations can either be cemented to the implants or screwed to the implants as conditionally removable dentures. While the cemented restorations can no longer be removed, the removal of conditionally removable prosthetic superstructures by the dentist is possible. Both principles of attachment are hotly debated and are part of many clinical studies and systematic reviews, the results of which are not uniform. In a systematic review, no differences in remodeling rates of crestal bone were found, depending on the type of fixation [47]. Also in terms of implant survival rates and prosthetic loss rates, no differences were found in a recent review [48]. The results of an earlier review point to the superiority of cemented superstructures in biological and clinical terms [49]. In contrast, in a recent systematic review of cemented total restorations, biological and / or technical complications were more commonly observed than with screwed full arch reconstructions [50]. However, screw retained ceramic supra-constructions had higher chipping rates of the veneers. In other systematic reviews, no differences in the survival rates of the implants and the superstructures depending on the type of fixation could be determined [48, 51]. It has to be taken into account that due to the sometimes very different study designs and in particular the different definitions of success parameters, a direct comparison of the two attachment types and evidence-based statements is currently not possible [52].
Conclusion
Ball type abutments (PS BA), Locator®-like abutments (PS Easy-Con) and MultiPlus attachments enable a reliable and predictable prosthetic restoration on four implants. The fact that a minimally invasive approach to implant placement was chosen in the present case increased the patient’s acceptance of the proposed implant therapy. The ability to target different prosthetic solutions with a reduced number of implants, depending on patient-specific factors, facilitates the implementation of patient desires, and allows redesign of the prosthetic solution even during ongoing therapy.
Literature:
- Gerritsen A. E., Allen P. F., Witter D. J., Bronkhorst E. M., Creugers N. H.: Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. Health Qual Life Outcomes 8, 126 (2010).
- Nordenram G., Davidson T., Gynther G., Helgesson G., Hultin M., Jemt T., Lekholm U., Nilner K., Norlund A., Rohlin M., Sunnegardh-Gronberg K., Tranaeus S.: Qualitative studies of patients’ perceptions of loss of teeth, the edentulous state and prosthetic rehabilitation: a systematic review with meta-synthesis. Acta Odontol Scand 71, 937-51 (2013).
- Armellini D. B., Heydecke G., Witter D. J., Creugers N. H.: Effect of removable partial dentures on oral health-related quality of life in subjects with shortened dental arches: a 2-center cross- sectional study. Int J Prosthodont 21, 524-30 (2008).
- De Bruyn H., Raes S., Matthys C., Cosyn J.: The current use of patient-centered/reported outcomes in implant dentistry: a systematic review. Clin Oral Implants Res 26 Suppl 11, 45-56 (2015).
- Emami E., Heydecke G., Rompre P. H., de Grandmont P., Feine J. S.: Impact of implant support for mandibular dentures on satisfaction, oral and general health-related quality of life: a meta- analysis of randomized-controlled trials. Clin Oral Implants Res 20, 533-44 (2009).
- Chen P., Yu S., Zhu G.: The psychosocial impacts of implantation on the dental aesthetics of missing anterior teeth patients. Br Dent J 213, E20 (2012).
- Warreth A., Alkadhimi A. F., Sultan A., Byrne C., Woods E.: Mandibular implant-supported overdentures: attachment systems, and number and locations of implants–Part I. J Ir Dent Assoc 61, 93-7 (2015).
- Johannsen A., Westergren A., Johannsen G.: Dental implants from the patients perspective: transition from tooth loss, through amputation to implants – negative and positive trajectories. J Clin Periodontol 39, 681-7 (2012).
- Trulsson U., Engstrand P., Berggren U., Nannmark U., Branemark P. I.: Edentulousness and oral rehabilitation: experiences from the patients’ perspective. Eur J Oral Sci 110, 417-24 (2002).
- Teofilo L. T., Leles C. R.: Patients’ self-perceived impacts and prosthodontic needs at the time and after tooth loss. Braz Dent J 18, 91-6 (2007).
- Brennan M., Houston F., O’Sullivan M., O’Connell B.: Patient satisfaction and oral health-related quality of life outcomes of implant overdentures and fixed complete dentures. Int J Oral Maxillofac Implants 25, 791-800 (2010).
- Pommer B., Mailath-Pokorny G., Haas R., Busenlechner D., Furhauser R., Watzek G.: Patients’ preferences towards minimally invasive treatment alternatives for implant rehabilitation of edentulous jaws. Eur J Oral Implantol 7 Suppl 2, S91-109 (2014).
- Al-Omiri M. K., Hammad O. A., Lynch E., Lamey P. J., Clifford T. J.: Impacts of implant treatment on daily living. Int J Oral Maxillofac Implants 26, 877-86 (2011).
- Walia K., Belludi S. A., Kulkarni P., Darak P., Swamy S.: A Comparative and a Qualitative Analysis of Patient’s Motivations, Expectations and Satisfaction with Dental Implants. J Clin Diagn Res 10, ZC23-6 (2016).
- Yao J., Li M., Tang H., Wang P. L., Zhao Y. X., McGrath C., Mattheos N.: What do patients expect from treatment with Dental Implants? Perceptions, expectations and misconceptions: a multicenter study. Clin Oral Implants Res, (2016).
- da Cunha M. C., Santos J. F., Santos M. B., Marchini L.: Patients’ Expectation Before and Satisfaction After Full-Arch Fixed Implant-Prosthesis Rehabilitation. J Oral Implantol 41, 235-9 (2015).
- de Siqueira G. P., dos Santos M. B., dos Santos J. F., Marchini L.: Patients’ expectation and satisfaction with removable dental prosthesis therapy and correlation with patients’ evaluation of the dentists. Acta Odontol Scand 71, 210-4 (2013).
- de Souza F. I., de Souza Costa A., Dos Santos Pereira R., Dos Santos P. H., de Brito R. B., Jr., Rocha E. P.: Assessment of Satisfaction Level of Edentulous Patients Rehabilitated with Implant- Supported Prostheses. Int J Oral Maxillofac Implants 31, 884-90 (2016).
- Kuoppala R., Napankangas R., Raustia A.: Quality of Life of Patients Treated With Implant- Supported Mandibular Overdentures Evaluated With the Oral Health Impact Profile (OHIP-14): a Survey of 58 Patients. J Oral Maxillofac Res 4, e4 (2013).
- Mumcu E., Bilhan H., Geckili O.: The effect of attachment type and implant number on satisfaction and quality of life of mandibular implant-retained overdenture wearers. Gerodontology 29, e618-23 (2012).
- Thomason J. M., Feine J., Exley C., Moynihan P., Muller F., Naert I., Ellis J. S., Barclay C., Butterworth C., Scott B., Lynch C., Stewardson D., Smith P., Welfare R., Hyde P., McAndrew R., Fenlon M., Barclay S., Barker D.: Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients–the York Consensus Statement. Br Dent J 207, 185-6 (2009).
- Mericske-Stern R., Worni A.: Optimal number of oral implants for fixed reconstructions: a review of the literature. Eur J Oral Implantol 7 Suppl 2, S133-53 (2014).
- Foundation for Oral Rehabilitation (FOR): Patient-centred rehabilitation of edentulism with an optimal number of implants. A Foundation for Oral Rehabilitation (FOR) consensus conference. Eur J Oral Implantol 7 Suppl 2, S235-8 (2014).
- Roccuzzo M., Bonino F., Gaudioso L., Zwahlen M., Meijer H. J.: What is the optimal number of implants for removable reconstructions? A systematic review on implant-supported overdentures. Clin Oral Implants Res 23 Suppl 6, 229-37 (2012).
- Pomares C.: A retrospective study of edentulous patients rehabilitated according to the ‘all-on- four’ or the ‘all-on-six’ immediate function concept using flapless computer-guided implant surgery. Eur J Oral Implantol 3, 155-63 (2010).
- Krennmair G., Seemann R., Fazekas A., Ewers R., Piehslinger E.: Patient preference and satisfaction with implant-supported mandibular overdentures retained with ball or locator attachments: a crossover clinical trial. Int J Oral Maxillofac Implants 27, 1560-8 (2012).
- Krennmair G., Seemann R., Weinlander M., Piehslinger E.: Comparison of ball and telescopic crown attachments in implant-retained mandibular overdentures: a 5-year prospective study. Int J Oral Maxillofac Implants 26, 598-606 (2011).
- Chiapasco M., Zaniboni M., Rimondini L.: Dental implants placed in grafted maxillary sinuses: a retrospective analysis of clinical outcome according to the initial clinical situation and a proposal of defect classification. Clin Oral Implants Res 19, 416-28 (2008).
- Misch C. E.: Divisions of available bone in implant dentistry. Int J Oral Implantol 7, 9-17 (1990).
- Misch C. E.: Density of bone: effect on treatment plans, surgical approach, healing, and progressive boen loading. Int J Oral Implantol 6, 23-31 (1990).
- Gambia. The World in Figures. London: Palgrave Macmillan UK; 1978. p. 69-.
- Alsaadi G., Quirynen M., Komarek A., van Steenberghe D.: Impact of local and systemic factors on the incidence of oral implant failures, up to abutment connection. J Clin Periodontol 34, 610- 7 (2007).
- Sclar A. G.: Guidelines for Flapless Surgery. Journal of Oral and Maxillofacial Surgery 65, 20-32 (2007).
- Allen F., Smith D. G.: An assessment of the accuracy of ridge-mapping in planning implant therapy for the anterior maxilla. Clin Oral Implants Res 11, 34-8 (2000).
- Wilson D. J.: Ridge mapping for determination of alveolar ridge width. Int J Oral Maxillofac Implants 4, 41-3 (1989).
- Esposito M., Hirsch J. M., Lekholm U., Thomsen P.: Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. Eur J Oral Sci 106, 527-51 (1998).
- Uludag B., Polat S., Sahin V., Comut A. A.: Effects of implant angulations and attachment configurations on the retentive forces of locator attachment-retained overdentures. Int J Oral Maxillofac Implants 29, 1053-7 (2014).
- Scherer M. D., McGlumphy E. A., Seghi R. R., Campagni W. V.: Comparison of retention and stability of two implant-retained overdentures based on implant location. J Prosthet Dent 112, 515-21 (2014).
- Seo Y. H., Bae E. B., Kim J. W., Lee S. H., Yun M. J., Jeong C. M., Jeon Y. C., Huh J. B.: Clinical evaluation of mandibular implant overdentures via Locator implant attachment and Locator bar attachment. J Adv Prosthodont 8, 313-20 (2016).
- Ceruti P., Menicucci G., Schierano G., Mussano F., Preti G.: Mandibular implant-retained overdentures with 2 different prosthetic designs: a retrospective pilot study on maintenance interventions. Int J Prosthodont 19, 557-9 (2006).
- Elsyad M. A., Mahanna F. F., Elshahat M. A., Elshoukouki A. H.: Locators versus magnetic attachment effect on peri-implant tissue health of immediate loaded two implants retaining a mandibular overdenture: a 1-year randomised trial. J Oral Rehabil 43, 297-305 (2016).
- Grey E. B., Harcourt D., O’Sullivan D., Buchanan H., Kilpatrick N. M.: A qualitative study of patients’ motivations and expectations for dental implants. Br Dent J 214, E1 (2013).
- Castillo-Oyague R., Suarez-Garcia M. J., Perea C., Rio J. D., Lynch C. D., Gonzalo E., Torres-Lagares D., Preciado A.: Validation of a new, specific, complete, and short OHRQoL scale (QoLFAST-10) for wearers of implant overdentures and fixed-detachable hybrid prostheses. J Dent 49, 22-32 (2016).
- Preciado A., Del Rio J., Lynch C. D., Castillo-Oyague R.: Impact of various screwed implant prostheses on oral health-related quality of life as measured with the QoLIP-10 and OHIP-14 scales: a cross-sectional study. J Dent 41, 1196-207 (2013).
- Rehmann P., Rudel K., Podhorsky A., Wostmann B.: Three-Year Analysis of Fixed and Removable Telescopic Attachment-Retained Implant-Supported Dental Prostheses: Survival and Need for Maintenance. Int J Oral Maxillofac Implants 30, 918-24 (2015).
- Kern J. S., Kern T., Wolfart S., Heussen N.: A systematic review and meta-analysis of removable and fixed implant-supported prostheses in edentulous jaws: post-loading implant loss. Clin Oral Implants Res 27, 174-95 (2016).
- de Brandao M. L., Vettore M. V., Vidigal Junior G. M.: Peri-implant bone loss in cement- and screw-retained prostheses: systematic review and meta-analysis. J Clin Periodontol 40, 287-95 (2013).
- Sherif S., Susarla H. K., Kapos T., Munoz D., Chang B. M., Wright R. F.: A systematic review of screw- versus cement-retained implant-supported fixed restorations. J Prosthodont 23, 1-9 (2014).
- Nissan J., Narobai D., Gross O., Ghelfan O., Chaushu G.: Long-term outcome of cemented versus screw-retained implant-supported partial restorations. Int J Oral Maxillofac Implants 26, 1102-7 (2011).
- Millen C., Bragger U., Wittneben J. G.: Influence of prosthesis type and retention mechanism on complications with fixed implant-supported prostheses: a systematic review applying multivariate analyses. Int J Oral Maxillofac Implants 30, 110-24 (2015).
- Wittneben J. G., Millen C., Bragger U.: Clinical performance of screw- versus cement-retained fixed implant-supported reconstructions–a systematic review. Int J Oral Maxillofac Implants 29 Suppl, 84-98 (2014).
- Ma S., Fenton A.: Screw- versus cement-retained implant prostheses: a systematic review of prosthodontic maintenance and complications. Int J Prosthodont 28, 127-45 (2015).